Dr. Anjonn Dasgupta
MBBS, MRCS, FRCS, PGDHA, PGDPC
CONSULTANT SURGEON
Important Case Studies


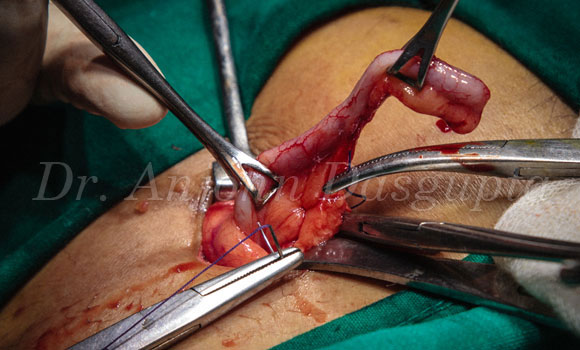



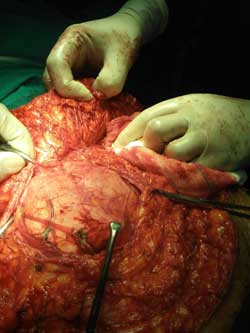
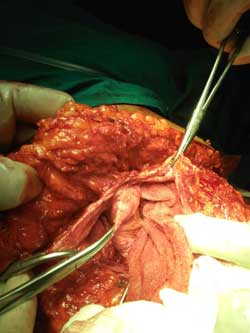
Case: Obstructed Paraumbilical Hernia
Operation for Obstructed Paraumbilical Hernia with inlay and onlay composite mesh and Abdominoplasty at the same sitting.




Case: 1
A 20 year old girl with 41 kg body weight presented with severe abdominal pain and huge abdominal distention. Was immediately admitted to a local facility and transferred to a higher centre when she showed signs of rapid deterioration and went in for a septic shock. She was misdiagnosed as a case of ectopic pregnancy, which was promptly ruled out by necessary investigations. She was taken for immediate surgical intervention and during anesthetic induction, she had a cardiac arrest. She was somehow revived, followed by operative intervention with a 100% mortality consent. She was diagnosed to have four large tears in her large intestine and had 4.5 ltrs of frank stool in her abdomen. She also had a huge mesenteric cyst turned abscess. The whole operation was done in a very short time with utmost precision as the patient was very unstable could have died on the table. A new port for passing stool (ileostomy) was done to keep the damaged area at rest. No portion of the large gut was excised and all the rents were sutured over patches of omentum. She was shifted to the ICCU and was managed as per critical care protocol and re-operated on two more occasions for management of burst abdomen and drainage of subcutaneous pockets of pus. There was no complication related to faecal fistula and she was discharged after about 40 days of tumultuous post-operative journey. She was ultimately proved to be having a dangerous stage of fulminant tuberculosis of intestine on biopsy and was treated conservatively for six months following which she was taken for a definitive surgery- closure of ileostomy, separation of all adhesions and bands and intestinal byepass and followed up with further anti tuberculosis management for a further period of one year. She has now matured into a beautiful 35 year old woman content in her own job and social pursuits.
Case: 2
A 55 year old female previously undiagnosed diabetic woman was presented with features of acute calculus cholecystitis (Gall Stone Disease). In view of developing sepsis, she was taken for urgent operation. She was diagnosed on table to have acute empyema gall bladder with around 300ml of frank pus and multiple stones inside gall bladder. A cholecystectomy was done and a thorough lavage of the abdominal cavity was carried out. She was shifted to ICU where she developed fulminant sepsis with acute renal failure and multi organ dysfunction syndrome in spite of being under very broad spectrum antibiotics. She was put on ventilator and went into coma and was shifted to a higher centre, had a horrendous post-operative period of 27 days, but she recovered well and was discharged in a stable condition.
Case: 3
BM a 33 year old lady from teaching profession presented with recurrent episodes of chest discomfort and had undergone repeated cardiologic assessments and she was already on a number of cardiac drugs. She had undergone cardiac angio which showed a muscle bridge and was scheduled for a repeat angio at Apollo Chennai for further management. At that point I had the opportunity of witnessing her distress and examined her. My clinical judgement was in favour of a non-functioning Gall Bladder which was later on proved partially on a radionucleide scanning. She was taken for operation and she was seen to have cholesterosis, a strawberry Gall Bladder and she got cured for life. She was taken off all cardiac drugs for the last 12 yrs.
Case: 4
RR, a 22 year old lady, mother of a year old child, presented in shock with collapse. She had no recordable BP and extremely feeble pulse and almost in respiratory failure. She was pale as paper. She had an abortion done at a well-known centre some 3 days back following which she progressively deteriorated and did not respond to conservative management. She was resuscitated for 10 hours following which she was taken for surgery with prior mortality consent. She was found to have a big rent in her uterus and multiple small & large tears in the large gut & small gut and that led to severe blood loss and faecal contamination of the abdominal cavity and went in complete hemodynamic collapse with severe septic shock. The bleeding tissues were repaired and the colonic tears & intestinal injuries were repaired and a de-functioning ileostomy was done to allow the tissue distally to heal. She had a horrendous post operation with multi-organ failure, received 10 units but responded favourably. She had multiple small corrective surgeries for post-operative infection and wound dehiscence etc. But ended up recovering well. She later develops a faecal fistula which was corrected later. She has now recovered completely into a healthy woman and is leading a normal life for the last 3 years.